Budget: whopping subsidies, private health profiteering as waiting lists rise

The health component of the budget focused on NDIS cost cuts. Not much has changed and fundamental flaws in the healthcare sector remain unresolved. Claudia Weisenberger reports.
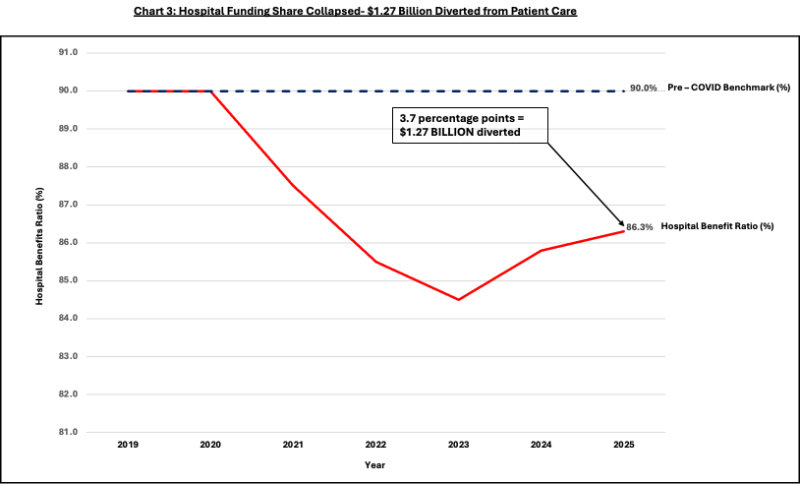
In 2023/24, major health insurers posted $2.11bn in pre-tax profits. APRA. The share of premium dollars reaching hospitals has fallen from 90% (pre-COVID) to approximately 84% by 2022/23; The latest data (December 2025) shows a modest improvement to 86.3%, still below the 90% standard.
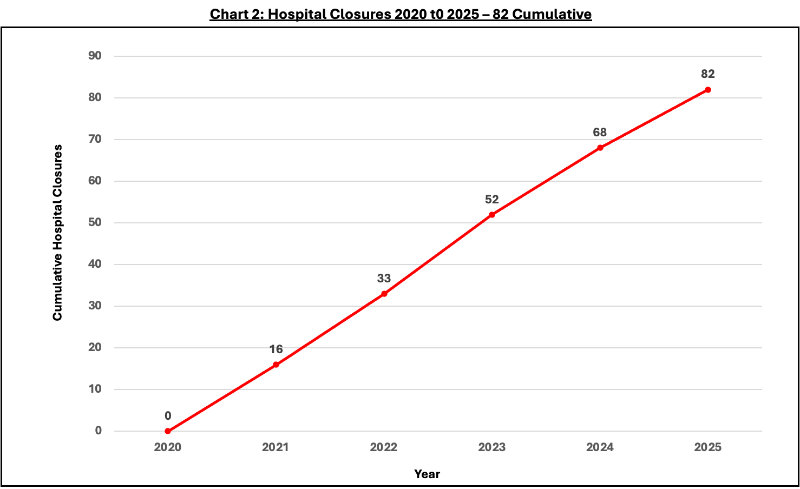
Public elective surgery waiting lists increased 41.6%.
Subsidies increased from $6.5B in 2022/23 to $6.9B in 2023/24 and $7.9B in this financial year; 23% increase from 2012-13 baseline.
Source: Australian Government Budget Papers 2012-13 to 2025-26.
Meanwhile, while insurers’ profits remain strong, the share of hospital funding remains below pre-COVID levels, and public waiting lists continue to grow as hospitals close.
Health insurance industry to protest discount changes as hospitals close
If increased subsidies do not prevent hospital closures, restore hospital funding rates, or ease public waiting list pressure, what policy goal justifies the spending?
opportunity cost
Every discounted dollar is a dollar that does not enable Australians to save on health or flow to public hospitals that serve all Australians, including the chronically ill, low-income and job-interrupted groups that the Private Health Association (PHA) invokes in advocating for social rating.
$7.9 billion is flowing into an industry that has made over $2 billion in profits while reducing hospital funding shares. Waiting lists in public hospitals increased by 433,000 patients. The equity question: Should the $7.9 billion continue to subsidize industry profits or allow for individual health savings while strengthening public capacity?
Source: Australian Private Hospitals Association.
Geographic distribution is important. A metropolitan day surgery is not a substitute for a regional full-service hospital. Lost service categories, including specialty maternity care predicted to disappear by the end of the decade, do not appear in facility counts.
PHA plays down hospitals’ claims of underfunding, but the numbers tell a different story.
Source: APRA Quarterly Private Health Insurance Statistics.
government evidence
The 2023 Finity report prepared by the Department of Health found that cutting rebates for over 65s would save $482 million in rebate costs, but $547 million would shift to the public system, a net loss.
Health Minister Mark Butler nevertheless rescinded these reductions, describing them as ‘unfair’, against the advice of his own department. This contradiction raises the real issue: not whether subsidies are necessary, but where the money goes.
When $7.9B yields $2B in profit as hospital shares drop from 90% to 86.3%, the question is allocation.
A reasonable next step would be the introduction of independent disclosure. A clear reconciliation of insurer-hospital funding streams, audited and published, mandatory publication of funding streams, premium-benefit ratios by tier and product, and data underlying disputed claims would resolve these questions once and for all.
What is ‘good’ value?
Do the $7.9 billion annual subsidies provide value commensurate with the cost?
Record profits, falling hospital shares, 82 closings and 41.6% growth in the waiting list are on top of a subsidy that increased by $1.5 billion from a 2012-13 baseline. Every dollar that subsidizes profits is a dollar that does not flow into the individual health savings that Australians have or into public capacity to serve the majority.
Singapore shows that health savings accounts, catastrophic insurance and robust safety nets deliver superior outcomes at lower costs.[7] Australia could direct some of the $7.9 billion to individual accounts while strengthening public capacity.
The question is not whether healthcare will be supported or not. It matters whether the current allocation serves Australians well. The numbers show that it is not.
Private health care. Why are community ratings failing teens?

Claudia Weisenberger is a management consultant with deep experience in pharmaceutical, hospital transformations and strategic due diligence on four continents. It combines keen analysis with hands-on application.




